- Follow Us :
24*7 Helpline
0154 2460722

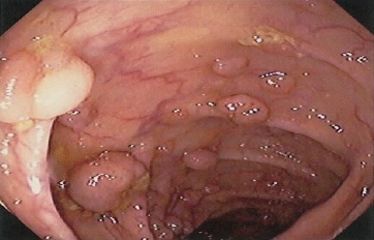
It used to be relatively simple for gastroenterologists to determine colonoscopy surveillance intervals when removing right-sided polyps: We considered whether the polyp was hyperplastic or adenomatous and its size. Now, we have a new classification system that includes adenomas, hyperplastic lesions, sessile serrated polyps (SSPs), and sessile serrated adenomas (SSAs) — all of which may require various surveillance intervals depending on their number and size. In my practice, I have noticed an evolution in my pathologist’s understanding of this new nomenclature, and in accuracy of reporting lesions — especially with regard to the important distinction between an SSP and an SSA. Early on, all sessile serrated lesions were being classified as SSAs despite these lesions being ...
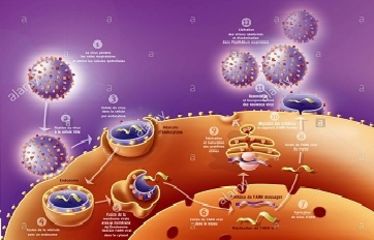
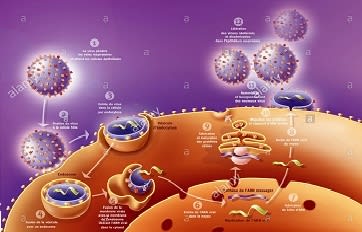
Recently, we have seen remarkable progress in the treatment of chronic infection with hepatitis C virus — from long courses of injectable interferon plus ribavirin to short courses of once-daily oral sofosbuvir. Not only have these shorter, more-manageable regimens proven more effective, they are substantially better tolerated. So, what’s the problem? It seems to be the price tag! Treating chronic HCV infection has never been cheap, but some of the newer treatments now cost over $80,000, and payers and patients are balking at the cost. Moreover, newer agents that may or may not be less costly will become available within the next year or so. So, I am curious to hear from you on the following: What is ...