- Follow Us :
24*7 Helpline
0154 2460722

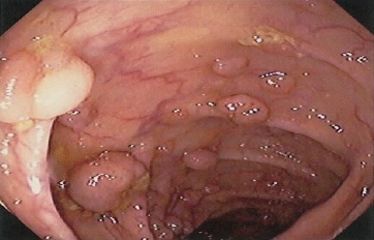
It used to be relatively simple for gastroenterologists to determine colonoscopy surveillance intervals when removing right-sided polyps: We considered whether the polyp was hyperplastic or adenomatous and its size. Now, we have a new classification system that includes adenomas, hyperplastic lesions, sessile serrated polyps (SSPs), and sessile serrated adenomas (SSAs) — all of which may require various surveillance intervals depending on their number and size. In my practice, I have noticed an evolution in my pathologist’s understanding of this new nomenclature, and in accuracy of reporting lesions — especially with regard to the important distinction between an SSP and an SSA. Early on, all sessile serrated lesions were being classified as SSAs despite these lesions being ...

Sometimes it’s because it was considered too “dangerous”. Occasionally it’s because “that’s not the way we do it”. Sorry, that doesn’t fly with me. And it shouldn’t with you. Yes, there are true medical reasons that some people shouldn’t have an upper endoscopy and a colonoscopy (sometimes called “bidirectional endoscopy” or a “double dip“) on the same day. But these are few and far between. Years ago, my mother told me the same thing…after her procedures. I nearly flipped out. The real reason is that (in the USA) the doctor and/or the facility gets paid less for doing them on the same day than when they do them on different days. ...